Cancer is a disorder of the DNA. The body has numerous defenses against cancer. A successful tumor must evade them all to become life threatening. Cancers are staged according to this success. Many cancers are curable if caught early.
This is 2nd in a 3 part series, discussing Cancer Diagnosis and Prognosis. The first in the series was Cancer Basic–Part 1–Initiation and Progression. Part 3 explains how various lifestyle choices can affect cancer.
Summarizing briefly, a cancerous cell is one that is proliferating uncontrollably due to DNA damage. Usually it is stem cells that become cancerous due to their inherent ability to divide.
A cancer must undergo a sequence of mutation to become dangerous. This varies from case to case, but here is a typical list
- A mutation in a cell’s DNA must happen.
- This mutation must cause uncontrolled division
- Cellular safeguards against such proliferation must be disabled.
- Programmed cell death – apoptosis – must be blocked.
- Cell senescence must be blocked.
- The mutation has to evade the immune system.
- To grow larger than a raisin, the cancer must develop a blood supply.
- The growing tumor must escape detection.
- The tumor must now metastasize and enter the blood stream.
- The cancer will have to evade detection in the bloodstream.
- The tumor must burrow back out of the bloodstream or lymph system and inflict itself on some other organ.
- Depending on where the metastatic tumor material landed, additional mutation may be needed.
Such a sequence seeme quite improbable, and it is. However, we have trillions of cells that could become candidates, so the improbable events do occasionally happen.
The Key Stages of Cancer
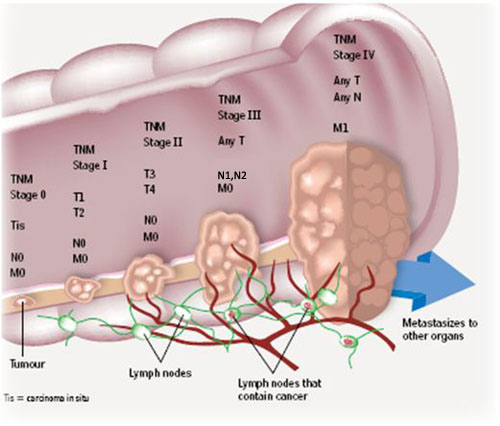 Cancer staging varies from cancer to cancer, and roughly reflects how far into the above sequence of mutations the cancer has traveled. A system in general use is the TNM system (also known as the UICC or AJCC system). TNM stands respectively for Tumor, lymph Node, and Metastasis.
Cancer staging varies from cancer to cancer, and roughly reflects how far into the above sequence of mutations the cancer has traveled. A system in general use is the TNM system (also known as the UICC or AJCC system). TNM stands respectively for Tumor, lymph Node, and Metastasis.
The T score identifies the size of the primary tumor. A following number indicates tumor size. T0 means no tumor found, with 1 through 4 indicating larger sizes. N0 means no spread to the nearby lymph nodes, and numbers 1-3 indicate the extent of the spread. Finally, M0 indicates no metastases, and M1 indicates some were found.
Many specific cancers use variants of this system, and some cancers use completely different systems. Breast cancer uses TMN and a I, II, III, & IV system as well. Colon cancer has an ABCD system as well as TMN.
Curing Cancer Requires Medical Intervention
A cancer that has gotten far enough to be detectable is not likely to go away on its own. It is possible, but bear in mind that a tumor large enough to be detected has probably gotten past the angiogenesis stage. This is a tumor on the march. Even with improvements in lifestyle, reversal is not likely. Because of this, by far the best chance is medical intervention. This can mean removal of the tumor by surgery or killing it in place with chemotherapy or radiation. Caught early, these therapies are very effective, and surgical procedures, radiation, and chemo are becoming far more precise and less destructive to surrounding tissue.
Catching a tumor early requires looking for it, and there is currently an unfortunate trend away from screening, a topic we will cover presently.
Early Detection is Extremely Important
If a tumor is detected, and is local, meaning it has not spread to the lymph node nor metastasized, recovery is highly likely for some cancers and less likely for others. Here are the odds of 5 year survival for several common cancers :
| Cancer Type | Localized | Spread to Lymph Nodes | Metastatic | Chance of getting it | Chance of dying from it. |
| Malignant Melanoma | 90% | 10% | 2.5% | 0.5% | |
| Squamous Cell Skin Cancer | ~100% | 10% | 7.5% | 0.01% | |
| Bladder Cancer | 88% | 55% | 15% | 2.5% | 0.6% |
| Breast Cancer | ~100% | 72% | 22% | 12% | 3% |
| Prostate Cancer | ~100% | ~100% | 28% | 15% | 2.6% |
| Colorectal Cancer | 92% | 65% | 11% | 4.6% | 1.9% |
| Esophageal Cancer | 40% | 21% | 4% | 0.9% | 0.7% |
| Lung Cancer | 31% | 15% | 2% | 6.8% | 5.8% |
| Pancreatic Cancer | 14% | 7% | 1% | 1.5% | 1.35% |
| Liver Cancer | 28% | 7% | 2% | ||
| Leukemia | Varies | Varies | Varies | 1.4% | 0.8% |
Now even with a ‘war on cancer’ that began 50 years ago, there is no clear evidence we are winning. Certainly there are breakthroughs, but people live longer, and can then get more cancer, plus heart disease is down and Adult Onset Diabetes is up, both of which tend to skew disease toward cancer. In fact, cancer is now the leading cause of death in America, UK and France.
But look at the above chart. Melanoma, breast cancer, prostate cancer, colorectal cancer, and bladder cancer are essentially curable if caught early. Nonetheless, they account for half the cancer deaths. Indeed a full 50% of cancer victims today may be dying needlessly.
Doesn’t this scream prevention – prevention – prevention? Yet the trend is clearly away from screening and little effort is in place to emphasize the role of prevention. A panoply of excuses are offered for this: not cost effective, stressful, over-treated etc. But this cut in the screening is a death sentence for a huge number of people.
If you have the ear of anyone influential, for the sake of all of us, bend it. We don’t need less detection. We need better processing of the results. Obviously.
Cancers That Can Be Detected While They Are Curable
These cancers are detectable at stages where they are still curable:
Colorectal. These are detectable with a colonoscopy, either a real one or a virtual one, which is slightly less unpleasant. This should start at 40. Forty year olds do not typically get colon cancer, but a full 20% of them have something pre-cancerous that ought to be closely watched. CEA, normally present only during a pregnancy, could indicate colorectal cancer. Change is important, so a history of the measurement should be maintained. CEA could also be present in people with breast, pancreatic, or lung cancer.
Breast Cancer. This is detectable by self-examination. 70-80% of cancers are, in fact, initially detected this way. Standard practice calls for mammograms. Mammograms have a ‘false alarm’ issue in that they detect ‘Ductal Carcinoma in Situ’ (DCIS) whish is really a pre-cancerous condition. Most, but not all DCIS goes away of its own accord. After any initial indication of a problem, the usual procedure is to follow up with MRIs, ultrasounds, biopsies, and other tests. As a preventive measure, insulin, IGF-1 and estradiol can be monitored. If these are in normal ranges and ratios, breast cancer risk is significantly reduced.
Prostate Cancer. This can be detected with a PSA measurement, a simple blood test. There are several other detection methods, including ultra sound, MRIs and biopsies. PSA alone is not a very good indicator. It is the rate of change that is important. For this reason, it is very desirable to have a series of measurements.
Squanous Cell Skin Cancer. Spotted as an abnormal skin growth.
Malignant melanoma. Any dark or mole like spot anywhere needs to be checked by a doctor.
Liver Cancer. AFP, a blood test, normally present only in pregnancy, could indicate liver or pancreatic cancer. Change is important, so a history of the measurement should be maintained. AFP could also be present in people with ovarian or testicular cancer. It is also often abnormal in fatty liver disease of alcoholic or non-alcoholic origin.
Ovarian cancer. CA125 may indicate ovarian cancer. Trend is more important than level, so it is important to have a series of measurements. CA-125 can be abnormal in endometriosis, early menopause of PCOS so always, and with everything, interpret with care. High AFP may also indicate ovarian cancer.
All except the skin cancers could show up on a full body scan. The resolution of such a scan is 3-4 millimeters. A tumor that size may have accomplished the angiogenesis step (growing a new blood supply), or not. If not, it is for the time being, stuck at that size. A targeted MRI has a finer resolution, and can get down to about a millimeter.
The Trend Away From Screening
This is thoroughly disturbing. Prostate cancer is a great example. The reasoning is that most men will get prostate cancer, but most  will not die from it, but when an elevated PSA is detected, men panic and opt for surgery. So we should stop detecting it? Perhaps we could instead persuade the eager surgeons and radiologists to refrain from rushing the patient into a lucrative surgery or other pricey procedure. Probably treatment is not necessary, but this can be monitored. Ignoring it solves nothing and sentences many to death. The other cancers seem to have similar screening stories. We will have more to say on this in the cancer sidebars.
will not die from it, but when an elevated PSA is detected, men panic and opt for surgery. So we should stop detecting it? Perhaps we could instead persuade the eager surgeons and radiologists to refrain from rushing the patient into a lucrative surgery or other pricey procedure. Probably treatment is not necessary, but this can be monitored. Ignoring it solves nothing and sentences many to death. The other cancers seem to have similar screening stories. We will have more to say on this in the cancer sidebars.
It may be the case that the trend away from screening has financial roots as well.
‘Miracle’ Cures Are Rare
 Miracle cures do happen. However, they don’t happen reliably. Otherwise they wouldn’t be considered miracles. They are very rare, something like 1 in 50,000 terminal cancers goes away. It makes for good stories, but not for good medicine. By far the best shot is with the medical experts. There has been progress and will be more. In fact, the grim survival odds presented above represent the past. There are already improvements that make the current prospects somewhat brighter.
Miracle cures do happen. However, they don’t happen reliably. Otherwise they wouldn’t be considered miracles. They are very rare, something like 1 in 50,000 terminal cancers goes away. It makes for good stories, but not for good medicine. By far the best shot is with the medical experts. There has been progress and will be more. In fact, the grim survival odds presented above represent the past. There are already improvements that make the current prospects somewhat brighter.
Given the curability of many of the more common cancers, it makes sense to screen early and often. Don’t let anyone convince you otherwise. Remind anyone that uses ‘cost effectiveness’ arguments that you are an individual, not a statistic, and that you and you alone can decide how much your health is worth. Insist on the tests. Waiting and hoping can be disastrous.
In Part 3, we will explain how lifestyle choices affect cancer incidence, and can lower recurrence rates should cancer be found, and, further, how to change and measure your lifestyle to maximize your protection against cancer.